.webp)
Introduction
She is 41. She sleeps seven hours and wakes up feeling like she did not sleep at all. She snaps at her husband over something trivial and feels genuinely horrified at herself an hour later. Her knees ache on the stairs. Her heart does a strange flutter during a meeting for no reason she can name. Her waist, which has never been a problem, has quietly expanded despite nothing changing in her diet. She Googles everything. Every search sends her to menopause content written for women in their mid-fifties. She closes the tab feeling like she is either too young for the answer or going quietly mad.
She is in perimenopause. And she almost certainly does not know it.
If you are a practitioner in India seeing women between 35 and 52, this is your most underprepared clinical encounter. If you are a woman reading this for yourself or for your mother, what follows is the framework that makes sense of what is happening and what can genuinely be done about it.
Perimenopause vs Menopause: The Distinction That Changes Everything
Most people understand menopause as the moment periods stop. What almost nobody explains is that the hormonal shift driving all the symptoms begins years and sometimes a full decade before that final period. That transition window is perimenopause, and it can start as early as the mid-thirties.
Menopause is technically a single point: twelve consecutive months without a period. Everything before that, while hormones are fluctuating and the ovaries are gradually producing less estrogen and progesterone, is perimenopause. Everything after is post-menopause. The language matters because the clinical picture differs in each phase, and the interventions should differ too.
In India, this conversation is largely absent from standard gynaecological care. Most women are told their symptoms are stress-related or that their blood work is normal. Many are offered antidepressants. The hormonal transition happening inside their bodies is not named, not explained, and not addressed. For a phase that can last eight to ten years, that is a significant failure.
What Are the Symptoms of Perimenopause? The Full Picture

The textbook symptoms such as hot flushes, night sweats, and irregular periods are well documented. What is not well documented, particularly in Indian clinical contexts, is the range of symptoms that arrive earlier and are far less commonly attributed to hormonal change.
Perimenopausal rage
This is real and it is physiological. The sharp, disproportionate irritability that many women describe is driven by progesterone decline, which reduces the calming effect on GABA receptors in the brain. It is not a personality problem. It is a neurochemical one.
Perimenopause brain fog
Brain fog like difficulty concentrating, losing words mid-sentence, forgetting names is one of the most distressing early perimenopause signs, and it is directly linked to estrogen's role in synaptic plasticity and cerebral glucose metabolism. When estrogen fluctuates, cognitive sharpness fluctuates with it.
Joint pain
Joint pain is poorly recognised as a perimenopause symptom in India. Estrogen has anti-inflammatory properties and maintains cartilage integrity. As levels drop, women notice aching in their knees, hips, and hands that is frequently misattributed to early arthritis or vitamin D deficiency alone.
Heart palpitations
Heart palpitations during perimenopause are common and largely benign, driven by estrogen's influence on the autonomic nervous system and cardiac rhythm. Cardiac investigations come back normal. The woman is told she is anxious. She is not anxious, she is in hormonal transition.
Perimenopause weight gain
Particularly the redistribution of fat toward the abdomen, is an almost universal complaint. The mechanism is a combination of rising cortisol, insulin resistance, declining estrogen (which shifts fat storage from hips to abdomen), and declining progesterone (which worsens fluid retention and blood sugar regulation).
Sleep disruption
Sleep distribution that is not explained by hot flushes is another early sign. Progesterone is a sleep-promoting hormone. As it declines, the architecture of deep sleep degrades. Women wake between two and four in the morning and cannot return to sleep.
Low mood and heightened anxiety
Anxiety and low mood in the perimenopausal window are frequently treated as de novo psychiatric conditions. They are not. They are downstream of progesterone decline, cortisol dysregulation, and disrupted serotonin-estrogen signalling.
The Cortisol and Estrogen Interplay Nobody Explains
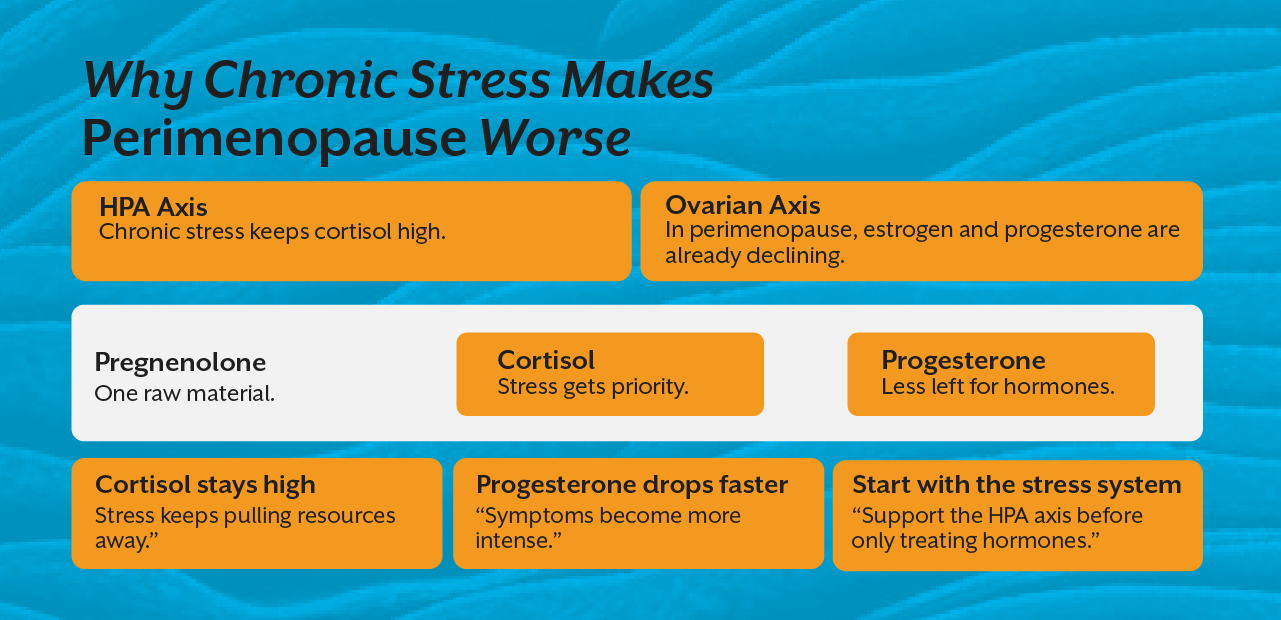
Perimenopause does not happen in isolation from the rest of the body's hormonal ecology. This is where perimenopause and cortisol become inseparable in any honest clinical conversation.
As ovarian estrogen and progesterone production becomes erratic in perimenopause, the adrenal glands are supposed to take up part of the slack. The adrenals produce a small but meaningful amount of estrogen and progesterone precursors, including DHEA, which can be converted peripherally. In a woman whose adrenal function is already compromised by years of chronic stress which describes a significant proportion of Indian urban women aged 35 to 50, this backup system is not available.
Meanwhile, cortisol and progesterone share the same precursor, pregnenolone. When cortisol demand stays elevated, progesterone production is further suppressed through the pregnenolone steal. The woman's already-declining progesterone drops faster. Her estrogen-to-progesterone ratio worsens. Symptoms intensify.
This is why perimenopause symptoms are so much more severe in women under chronic stress. The stress is not a trigger, it is an active biological driver worsening a hormonal transition the body was already managing on reduced capacity.
For practitioners, this means perimenopause functional nutrition cannot begin with the ovaries. It has to begin with the HPA axis. You cannot rebuild estrogen and progesterone balance while cortisol demand remains unchecked.
Understanding these interconnections in full depth like how the HPA axis, estrobolome, and sex hormones talk to each other across a woman's reproductive life is exactly the kind of systems framework covered in the Women's Hormonal Health course at iThrive Academy.
The Functional Nutrition Protocol for Perimenopause
Perimenopause natural remedies in India tend to be either Ayurvedic generalisations or generic wellness advice lifted from Western sources and poorly adapted to Indian food culture. What follows is neither.
Blood sugar regulation is the foundation
Insulin resistance accelerates in perimenopause due to declining estrogen's effect on insulin receptor sensitivity. Every meal that spikes blood sugar worsens the hormonal environment. The practical application in an Indian diet context is meaningful: reducing white rice portions and replacing some of the refined carbohydrate load with dal, vegetables, and adequate protein at each meal. Protein targets of 1.2 to 1.6 grams per kilogram of body weight support muscle preservation, metabolic rate, and hormone synthesis simultaneously.
Phytoestrogens deserve more clinical attention than they receive
Flaxseeds, sesame, and fermented soy provide lignans and isoflavones that weakly bind estrogen receptors and may buffer the estrogen fluctuation characteristic of early perimenopause. These are not hormones. They are modulators, and the evidence for symptom reduction, particularly hot flushes and mood instability is reasonably consistent.
Gut health directly influences hormonal clearance
As covered in detail in our earlier piece on female hormone health and the estrobolome, the composition of the gut microbiome determines whether estrogen is eliminated or reabsorbed. In perimenopause, supporting gut diversity through adequate fibre, fermented foods, and minimising antibiotic overexposure is not supplementary, rather it is mechanistically central.
Adrenal support through nutrition
Adequate dietary fat including saturated fat from ghee and coconut in traditional Indian cooking is essential for steroid hormone synthesis, including the adrenal production that becomes more important as ovarian output declines. Chronic low-fat dietary patterns in perimenopausal women are clinically counterproductive. Magnesium-rich foods including nuts, seeds, and dark leafy greens support both cortisol regulation and sleep architecture.
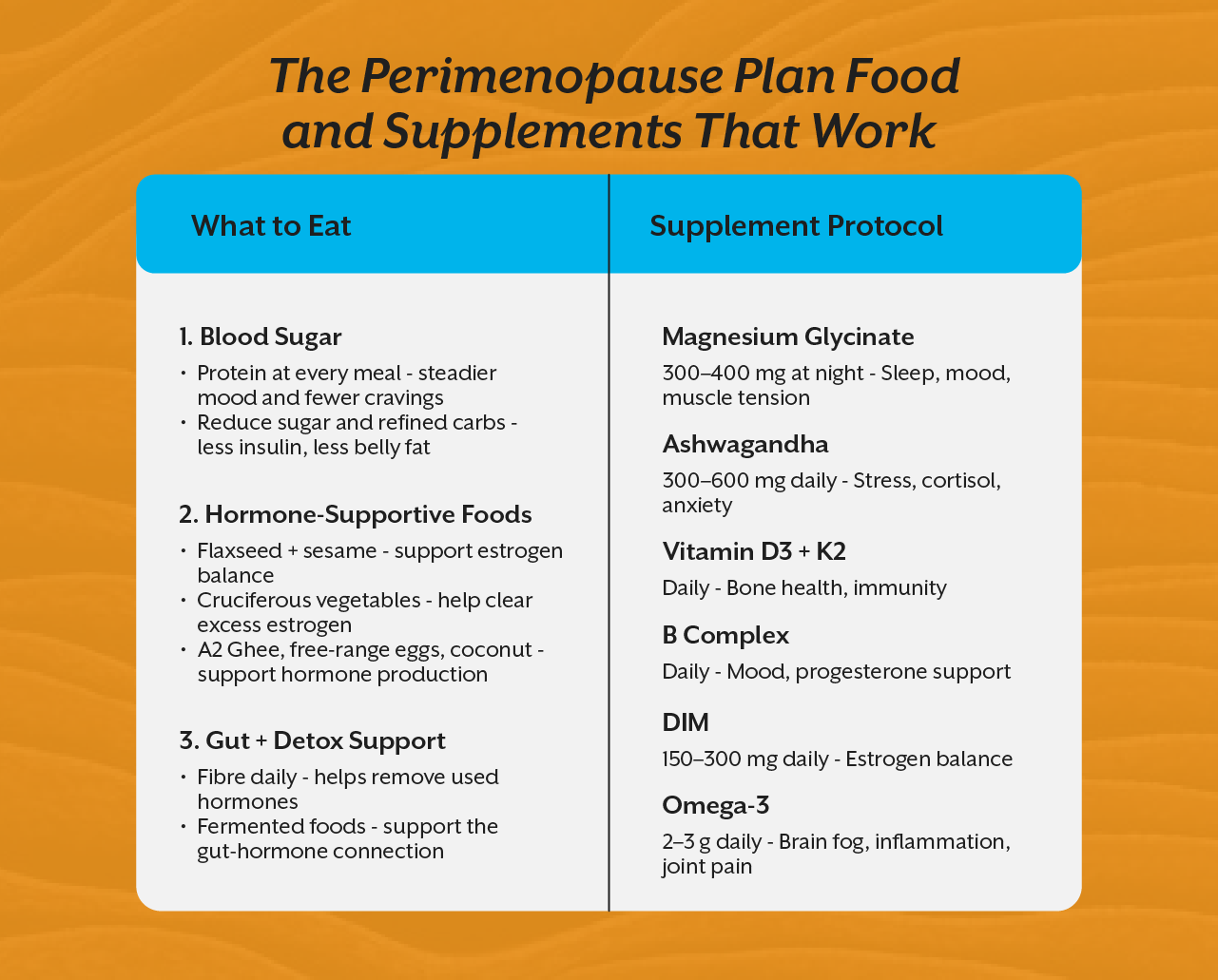
The Supplement Protocol Worth Knowing
Magnesium Bisglycinate
Magnesium Bisglycinate at 300 to 400mg at night addresses sleep disruption, mood instability, cortisol dysregulation, and muscle cramping simultaneously. It is arguably the single highest-yield supplement in perimenopause.
Ashwagandha
Ashwagandha as an adaptogen reduces cortisol output, supports adrenal reserve, and has specific evidence for reducing anxiety and improving sleep quality in perimenopausal women.
Vitamin D3 with K2
This addresses the bone density concern that begins in perimenopause well before menopause and is poorly recognised as a perimenopausal issue in Indian clinical practice.
B complex
B Complex supports progesterone production, serotonin synthesis, and the methylation pathways that process both estrogen and neurotransmitters.
DIM (diindolylmethane)
It supports estrogen metabolism through the safer 2-hydroxy pathway, reducing the estrogen dominance pattern that characterises early perimenopause.
What This Transition Deserves
Perimenopause is not a disease. It is a biological transition that, when supported correctly, does not have to be the decade of suffering that many Indian women normalise and endure silently. The difference between a woman who navigates this transition with relative stability and one who struggles for years is almost entirely a function of whether she has clinical support that understands what is actually happening hormonally.
That support begins with practitioners who are trained to see the full picture, and not just FSH and estradiol, but cortisol curves, DUTCH hormone metabolites, gut microbiome function, and the nutritional status that determines whether the body has the raw material to manage the transition at all.
If you want to build that level of clinical fluency, the iThrive Certified Functional Nutrition programme develops it through 12 modules of live, mechanistic clinical training built from the same practice that has helped over a thousand practitioners across India give their female patients the answers they have been waiting years to hear. The full ecosystem of courses, tools, and clinical frameworks lives at iThrive Academy.




.jpg)